What is it?
The Scaphoid is one of the eight carpal bones that make up the wrist. It is the commonest carpal bone to be fractured and is more common in young men. The injury occurs often from a fall onto an outstretched hand, sports related injury or a sudden torque injury from power tools. Scaphoid fractures tend to cause swelling and pain on the radial (thumb) side of the wrist and can often be overlooked as a wrist sprain. Despite seeking medical attention, there is a high rate of missed diagnoses due to many fractures not easily seen on initial X-Ray. The scaphoid has an unusual blood supply which can affect it’s healing. It is the key bone that stabilises the wrist and if a fracture is missed or does not heal, this can lead to collapse and arthritis in the wrist at an early age. If you have pain on the radial side of the wrist following an injury that continues for longer than a week, you should seek medical attention.
How should it be treated?
If initial X-Rays do not show the fracture but there is persistent pain and swelling in the radial side of the wrist, your doctor may ask you to have a CT or MRI scan to give more detailed imaging of the area. This can identify occult scaphoid fractures and the amount of displacement or other injured structures in the area such as distal radius fractures, scapholunate ligament injuries, trapezium fractures or other ligamentous injuries. This helps guide you and your doctor’s choice of treatment.
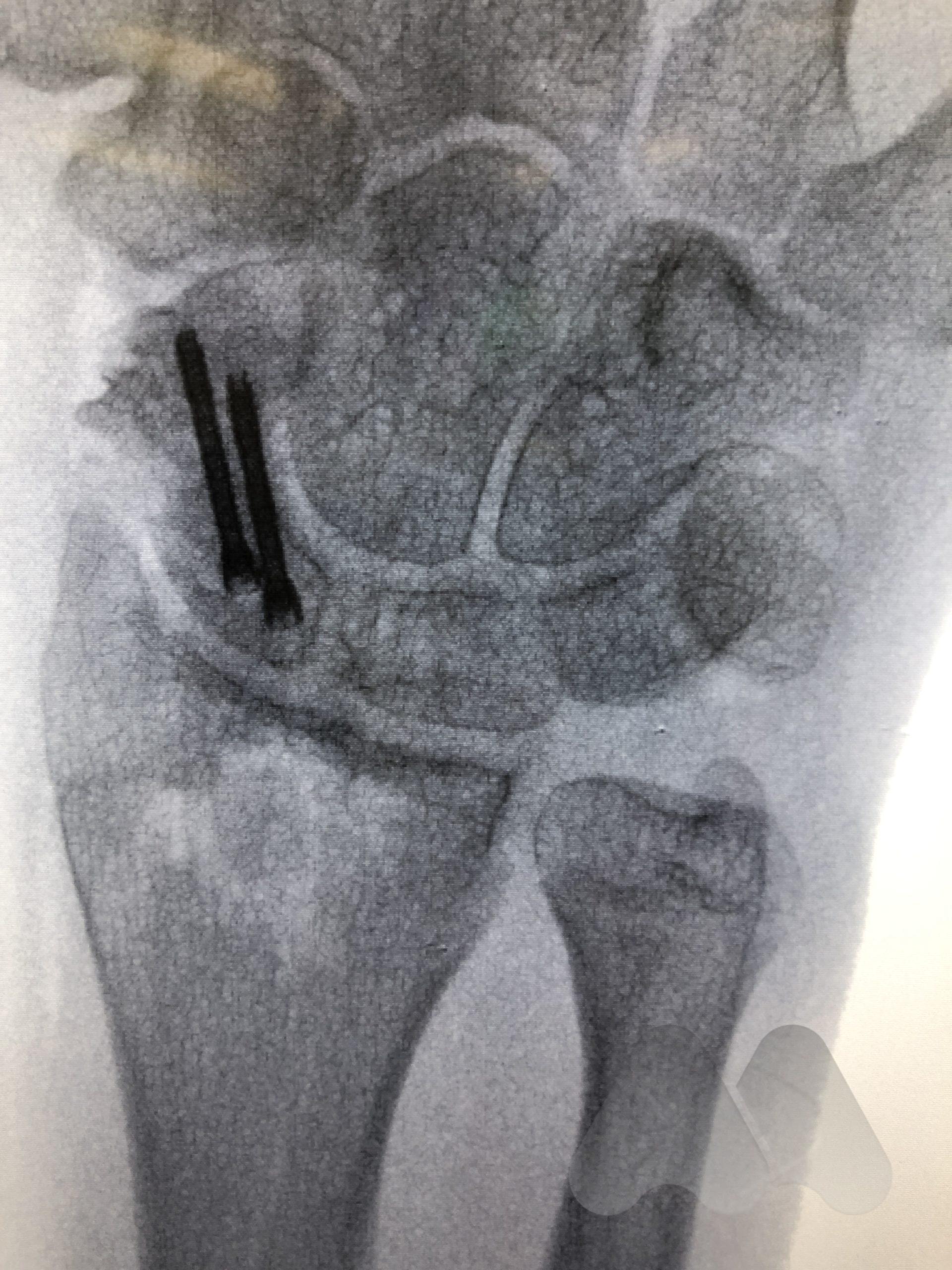
Undisplaced scaphoid waist and distal pole fractures have the best capacity to heal and have a >94% chance of healing even without surgery. They can be managed in a full-time cast or splint for eight weeks. Proximal pole fractures and those that are displaced have a higher risk of the fracture not healing. Proximal pole fractures have a 66% chance of healing by cast treatment and >1mm displacement at the waist, can reduce the healing rate to 73%. In these situations or where full time casting for eight weeks is not desirable, surgical fixation is an option to increase the chance of fracture healing. Depending on the location of the fracture, whether it is fragmented or displaced, will determine how the fracture is fixed. The most common type of fixation is by screw fixation buried inside the bone, inserted through a small incision on the palm near the thumb or back of the wrist.
In situations where scaphoid fractures have been initially missed but identified later, before the onset of arthritis, the diagnosis of a scaphoid non-union is made. These situations often require surgery as the chance of healing by late casting is unlikely to result in fracture healing. The surgery aims to clear out the scar tissue at the fracture site and sometimes add fresh bone from either the wrist or hip to add structural support and fill in defects in the bone and insert a screw for fracture fixation to get the bone to heal and restore normal stability to the wrist. The long term aims are to try and slow the progression towards arthritis in the wrist, however, research studies have shown that this can still develop. In some circumstances where the quality of the bone is poor or has lost it’s blood supply, bone graft with it’s own blood supply is taken from the wrist or knee and connected to the scaphoid.
What are the risks of surgery?
Surgery to fix scaphoid fractures is not without risk. There is still a risk that the fracture does not heal, with the highest risk in fractures that have been missed many months to years ago and those affecting the proximal pole where the blood supply has been lost and the bone is dead and can be up to 20% risk of non-union in some studies. Other risks include infection at the surgical site, stiffness in the wrist, irritation of cartilage from prominent screws or complications from the bone graft donor site.
What should I expect following surgery?
Surgery for scaphoid fracture fixation including bone grafting is often performed as day case surgery in hospital under a general anaesthetic. After surgery, you will be in a backslab for 1 week before having your wound checked and then changed into a thermoplastic splint by the hand therapists. Keeping your hand elevated above the level of your heart, ice to the back of the wrist and regular simple painkillers are effective ways of reducing the pain and swelling in the first 3-5 days following your operation. In addition to this, you may be prescribed some stronger painkillers for the first few days. Normally, you will be able to start moving your wrist after 1 week but should avoid carrying any load or strong gripping of the affected hand for the first 6 weeks. At 6 weeks you will have an X-Ray to confirm healing is progressing as expected and a CT scan to confirm the scaphoid is healed at 3 months following surgery. Common restrictions following surgery are the inability to drive or play sport for 6 weeks, returning to office duties at 1-2 weeks and manual labour at 6-8 weeks.