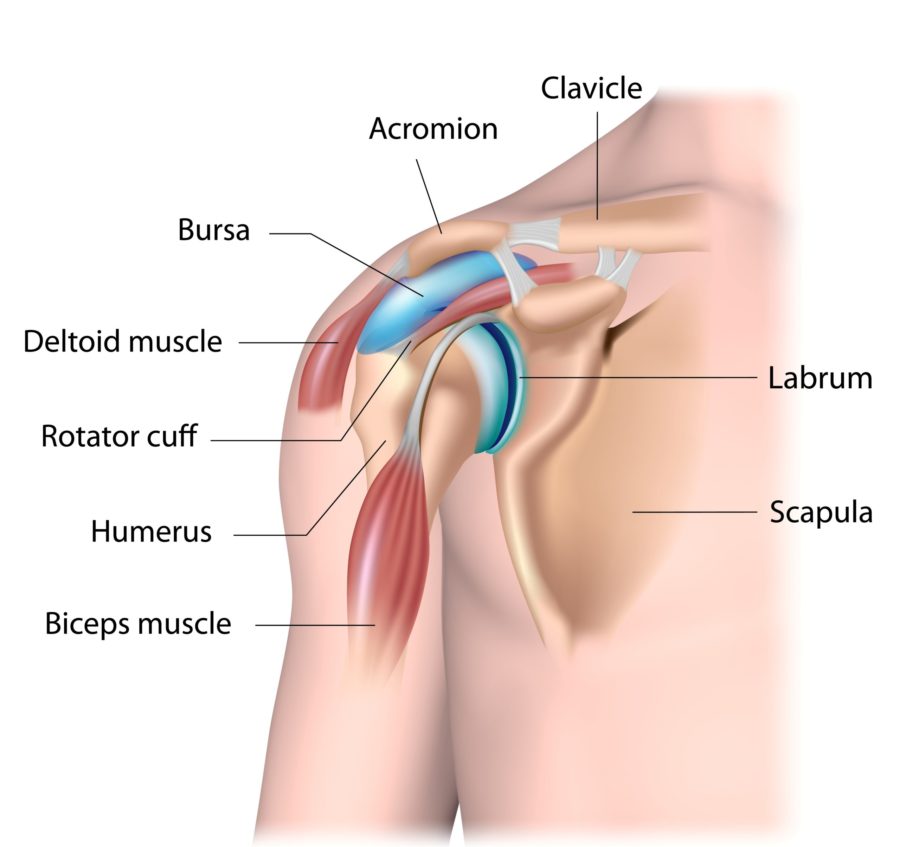
What is the rotator cuff?
The rotator cuff is a group of four tendons that connect the muscles of the shoulder blade to the top of the arm bone (humerus). They are responsible for the coordinated movements of the ball and socket of the shoulder joint that provides a a flexible range of of movement and strength. The tendons travel under an arch-like projection of bone of the shoulder blade called the acromion. Between the tendons and the acromion is a normal subacromial bursa which allows smooth gliding of the tendons as the shoulder moves.
What can go wrong with the rotator cuff?
Rotator cuff disease is the most common cause of shoulder pain. It encompasses a wide spectrum of degenerative and traumatic conditions affecting the shoulder joint. It includes:
- Subacromial bursitis and impingement – poor rotator cuff control that leads to inflammation of the bursa
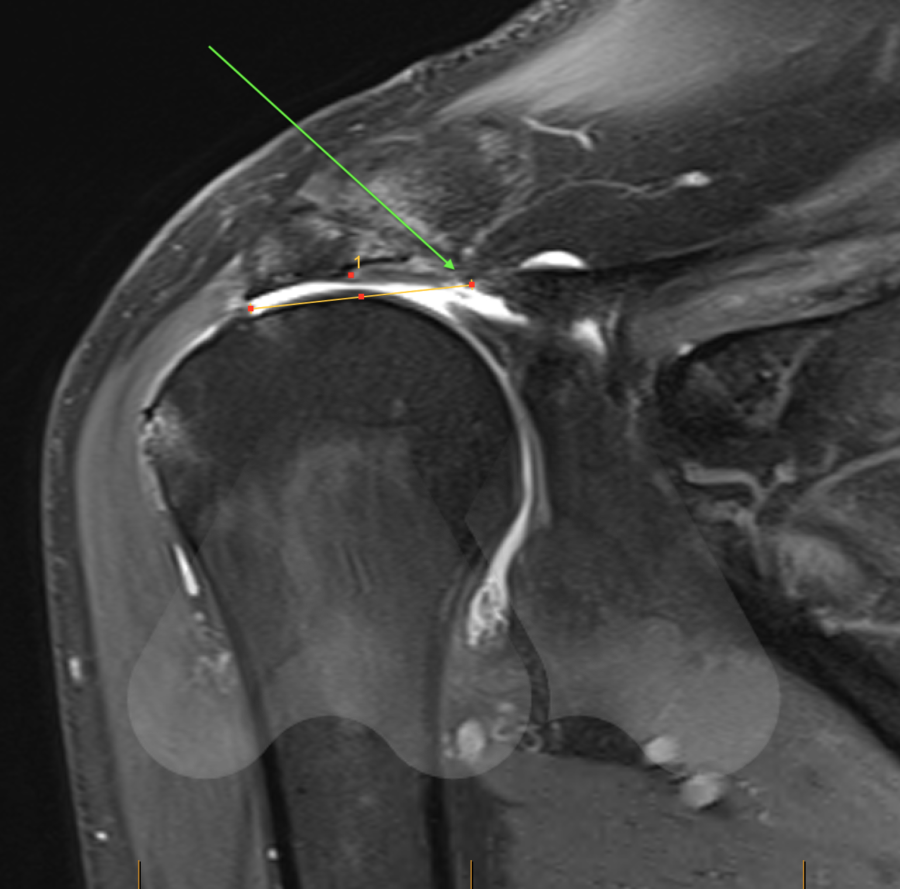
- Partial thickness and full thickness degenerative rotator cuff tears – accumulated damage of ageing tendons which may or may not cause pain
- Traumatic rotator cuff tears – Tear in a previously normal healthy rotator cuff
- Rotator cuff arthropathy – Shoulder arthritis due to long standing untreated rotator cuff tears
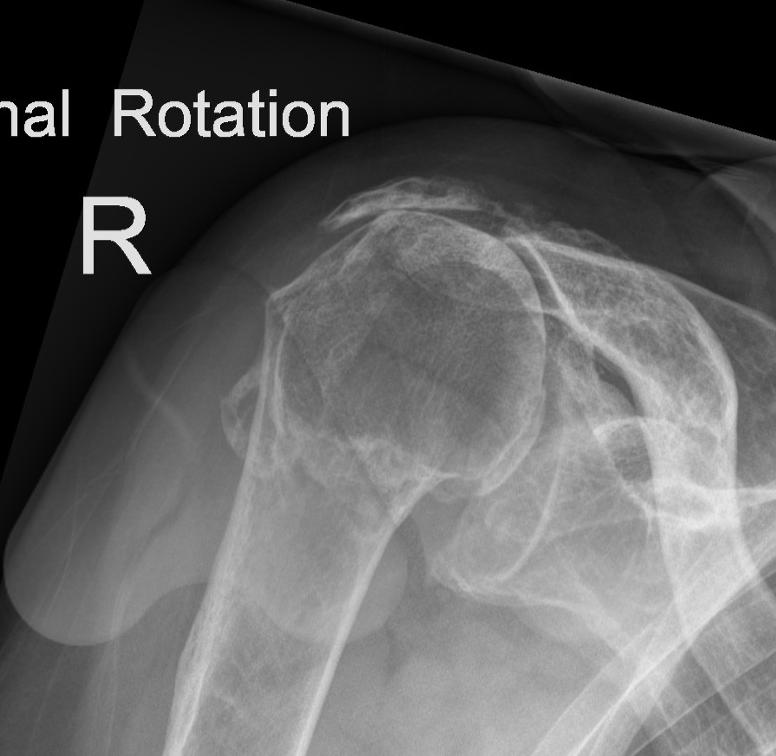
How do I know if I have a torn rotator cuff?
You may notice pain in the outer part of the shoulder that can radiate down the arm and can be worse at night time. You may also notice your arm to be weaker. Symptoms can be aggravated by overhead activity such as taking a mug from a top shelf or lifting objects away from the body such as lifting shopping bags into the boot of a car.
How should rotator cuff tears be treated?
There is a widely varied opinion on how rotator cuff tears, in particular, are managed and this is based on the following questions:
- Why are some rotator cuff tears asymptomatic
- What is the natural progression of rotator cuff tears if left untreated?
- Which asymptomatic rotator cuff tears are likely to become symptomatic?
- Which patients are best treated with rotator cuff repair?
Extensive research, to investigate these questions has been conducted. This evidence is the basis of how we educate patients and make decisions about how best to manage this common problem.
Asymptomatic patients with rotator cuff tears
13% of asymptomatic 50-60 year olds will have a full thickness rotator cuff tear. As we get older, the rotator cuff tendons weaken and are prone to tearing. If the remaining tendons and muscles around the shoulder are able to compensate for this slow weakening and tearing of the tendon, then patients may not feel pain. Upto 51% of asymptomatic patients over the age of 80 years old will have a full thickness rotator cuff tear.
What treatments are available?
Physiotherapy
Most patients (80%) with symptomatic degenerative rotator cuff tears can be treated with physiotherapy and avoid the need for surgery.(3) Physiotherapy is an effective treatment for sub-acromial bursitis and impingement. Treatment involves improving control of the shoulder blade, improving coordination and control of the intact remaining rotator cuff muscles as well as improving core muscle strength in the trunk.
Successful treatment with physiotherapy is not related to initial levels of pain, tear size or retraction or weakness in the shoulder.(3)
Rotator cuff repair
Rotator cuff repair can be performed by key-hole or mini-open techniques to repair the torn tendon back to the top of the humerus (arm bone).
Younger patients with higher activity levels may benefit from surgery. Research studies have shown that patients undergoing a rotator cuff repair for a small to medium sized full thickness tear, have greater improvements in function, satisfaction and shoulder strength compared with patients treated with physiotherapy. (5)
Success rates of healing of an isolated supraspinatus repair has been shown to be more than 80% when followed to 10 years. Interestingly, failed repairs, with an MRI or ultrasound finding of retear, do not correlate with patient satisfaction, pain levels or function. Factors that affect tendon healing rates include age, tear size and fat changes in the muscle that occur in long standing rotator cuff tears. (4)
Other surgical treatments for rotator cuff tears include:
- Tendon transfer surgery
- Superior capsular reconstruction
- Reverse total shoulder replacement